Q&A Library: The Multi-Step Shoemaker Protocol™ Breakdown and Lowdown
Is there a hack?
What is the minimum testing and steps needed?
Are there substitutes or variations?
“Climbing the pyramid step by step results in a progressively smaller number of people experiencing illness. Each step sequentially addresses a different abnormality in the body, revealing the necessary findings for treatment. We cannot determine if we have reached the "final" step until we actually take it.”
~ Dr. Ritchie Shoemaker
To address questions about shortcuts or alternatives in recovering from Chronic Inflammatory Response Syndrome (CIRS), it is crucial to recognize its complexity.
The Shoemaker Protocol™ provides a detailed step-by-step approach to overcoming CIRS and mold illness. It’s important to understand that CIRS caused by exposure to water-damaged buildings (WDBs) is not “just” an allergy or toxicity; rather, it is a multi-symptom, multi-system illness.
For most individuals, it is set off by a genetically predisposed condition that hampers the body’s ability to eliminate the biotoxins present in a WDB. When this condition becomes active, it leads to inflammation and various downstream effects throughout the body, each of which is addressed in the multi-step Protocol. If your case doesn’t reach recovery in the initial steps—and most do not—you will continue to advance through the Protocol steps, until your system reaches the highest level of recovery as indicated by proper testing.
As you continue through the Protocol steps, each one requires dedicated time and attention. There are no unnecessary steps. There are also nuances and tips associated with each step, and each specific case, which the Protocol and Shoemaker Protocol™ trained practitioners are designed to address comprehensively.
The steps of the Shoemaker Protocol™ offer not a “hack,” but the essential, strategic approach to address each aspect of the illness. The shortcut may simply be that you only need the first few steps. A high percentage of CIRS-diagnosed patients, however, do need to follow the Protocol through all the steps.
The Protocol treatment offers a health optimizing, synergistic blend of prescription medicine, detoxification, supplementation, diet, hormone regulation, etc., as needed at each step. By familiarizing yourself with the steps (included below), you will be able to get an idea of how this revolutionary Protocol comprehensively supports each aspect of recovery.
For those who need it, the last step, the VIP (vasoactive intestinal polypeptide) treatment, is a pinnacle step with marked results! At this end point of the journey it has the ability to correct the important biomarker abnormalities, and also to restore the regulation of the innate immune system.
**It is important to note, VIP will not be effective for these patients until they reach this final step. Specific criteria must be met prior to beginning VIP, then monitored.**
This is exciting news for even the most dire of cases. By dedicating yourself to the Shoemaker Protocol™, you're on a path to remarkable results. Thousands of patients, plus published, peer-reviewed studies support its effectiveness, so you can feel confident in this journey toward recovery and health.
INDEX:
SECTION 1: 12-Step Shoemaker Protocol™ step-by-step overview
SECTION 2: Q&As – Shortcuts, self treatment, minimum testing, duration of treatment, and more
SECTION 3: Q&As - Alternative testing, treatments, supplements
SECTION 4: 4 DIY Quick Start Steps & Symptom Roster
SECTION 5: Recommended Resources
SECTION 1: The 12-Step Shoemaker Protocol™ Summary
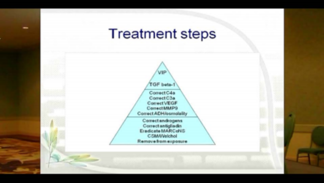
The Protocol initiated by Dr. Shoemaker is straight forward, but there are a series of steps to be taken, each in its sequential order. The idea is that these treatment steps are similar to how one would climb a pyramid.
If the patient shows through appropriate testing to be recovered with simple removal from exposure, no more steps are needed. However, it is important to note, there are few people with CIRS-WDB who recover with this step alone.
No single test, step, or intervention is likely to correct all the underlying abnormalities in the multiple inflammatory and immunological responses of CIRS. The Shoemaker Protocol™ treatments and their outcomes have been well-documented, reviewed, and proven time and again.
This treatment pathway offers a comprehensive, synergistic blend of prescription medicine, supplementation, diet, hormone regulation, etc., as needed for optimal recovery at each step.
With understanding of both CIRS and the Shoemaker Protocol™, it becomes clear how this proven pathway treats not symptoms, but targets each and every underlying cause of the illness, which in turn relieves and restores the downstream effects. Your path may end at step 3,6, or 12. You won’t absolutely know until you follow the proven treatment pathway here for you.
1/ Prove there is a multi-system & symptom illness due to exposure to a water damaged building.
A/ Find and test the water-damaged building affecting you.
For building diagnosis, test the building with ERMI or HERTSMI-2 dust or Swiffer testing (available at EnviroBiomics Labs). This will provide information about the biotoxins and levels you’ve been exposed to. It will also inform the remediation process.
B/ Prove there is a multi-symptom, multi-system illness
First, review the common symptom roster (see below) and confirm you have several common symptoms. See a more expanded roster in the Shoemaker Protocol™ Quick Start Guide.
Second, take the online Visual Contrast Sensitivity (VCS) test to confirm CIRS.
Next, establish care with a practitioner versed in the Shoemaker Protocol™, and proceed with a definitive diagnosis. This will include a detailed intake with history and a physical exam. Specific diagnostic tests are taken and reviewed establishing biomarkers, genetic susceptibility, and more.
2/ Correction of toxin overload using CSM and or Welchol as binders, plus VCS monitoring to assess progress.
The Visual Contrast Sensitivity test confirms resolving inflammation as the toxin levels drop.
3/ Eradicating biofilm-forming MARCoNS (with EDTA chelating spray).
If you find you still need to continue up the pyramid, the next step is the eradication of bacterial MARCoNS (Multiply Antibiotic Resistant Coagulase Negative Staphylococcus) from the nasopharynx, if present. These bacteria form a biofilm making it hard for many antibiotics to penetrate, sheltering the bacteria. Further, they are resistant to at least two classes of antibiotics. MARCoNS rarely exist if a patient has a normal MSH (melanocyte stimulating hormone), but normal MSH is unusual in CIRS patients.
To treat MARCoNS, a combination of therapies is used, including EDTA chelating spray. The EDTA clears the way for normal nasal flora to eradicate the MARCoNS.
This is an evolving aspect of microbiology as MARCoNS rapidly acquire resistance, especially when drugs like the antifungals used in the past create resistance.
4/ Correction of antigliadin antibodies by eliminating gluten for those with anti-gliadin positivity as shown by a positive blood test.
The fourth step is correction of antigliadin antibodies. Avoiding gluten allows the antibodies to levels to fall so inflammation will improve.
Many, but not most, patients will have a positive antigliadin antibody (AGA) in their initial lab work. When Celiac Disease is ruled out, treatment of patients consists of a gluten-free diet for three months followed by retesting. If the AGA is negative on retesting, gluten can often be reintroduced into the diet without consequences.
5/ Correcting abnormal androgens
The fifth step is correction of abnormal androgens typically caused by an up-regulated aromatase enzyme. Tailored to the specific case, treatment may consist of DHEA (dihydroepiandrosterone, a endogenous steroid hormone precursor, one of the most abundant circulating steroids in humans. DHEA is produced in the adrenal glands, the gonads, and the brain. It functions as a metabolic intermediate in the biosynthesis of the androgen and estrogen sex steroids), HCG (human chorionic gonadotropin) injections (or sublingually) for 5 weeks, or VIP (vasoactive intestinal polypeptide) nasal spray for 30 days, tailored to the patient’s condition and circumstances.
6/ Correcting ADH/osmolality
Step 6 is to correct antidiuretic hormone/osmolality problems, which often cause dehydration, thirst, frequent urination, headaches, and static shocks. Treatment consists of DDAVP, desmopressin (a synthetic form of the vasopressin hormone) tablets or nasal spray every other night for 10 nights. If you have correction of this quickly, there is no need to continue but many people will need to have daily desmopressin for approximately one month. Osmolality needs to be closely watched.
7/ Correcting MMP-9 with Omega 3s, plus the “No Amylose Diet”
The seventh step is to correct MMP-9, an inflammatory marker. This treatment entails using omega 3 fatty acids, usually EPA and DHA, in conjunction with a No Amylose Diet for the same time period.
The No Amylose Diet was developed by Dr. Shoemaker to help people with mold illness who have high levels of MMP-9. Cutting back on amylose, a carbohydrate found in mainly in starchy foods that grow underground like potatoes, sweet potatoes, peanuts, carrots, plus cereal grains, works to lower MMP-9 levels and inflammation.
8/ Correcting low VEGF (a signaling protein) with the no-amylose diet and a high dose omega 3
During this step we follow low VEGF (vascular endothelial growth factor, a signaling protein that promotes the growth of new blood vessels).
People won’t have symptomatic improvement if VEGF is below 31.
In CIRs, VEGF can be so low there is no way to increase blood flow during exercise, which results in persistent fatique, muscle aches and cognitive problems.
Correcting low VEGF involves the no amylose diet and high dose omega 3’s as before for MMP9 correction.
9/ Correcting elevated C3a with statins and CoQ10
Step 9 is the correction of high C3a. High dose statins are used to clear elevated C3a. Co-administration of CoQ10, beginning 10 days before starting the high dose statins will help prevent CoQ10 deficiency secondary to decreased HMG-CoA reductase function.
10/ Next, check for elevated C4a
This split product of the MBL (mannose binding lectin) pathway of the complement system is a key marker of how severe a patient’s CIRS (still) is. In the past we could use Procrit to correct C4a, but the FDA has put a black box on erythropoietin use. Because it’s not available, we move on with the C4a test results and follow the rest of the Protocol through to the final VIP step, as needed.
11/ Reducing elevated TGFB1 with Losartan
Step 11 is the correction of TGFB1 (transforming growth factor beta 1) an innate immune cytokine which is also a key marker of illness severity. It causes dysfunctional changes in tissues, lowers VEGF, and stimulates auto-immune issues. This protein generally falls as inflammation improves. If it is still elevated, it can be treated at this point with Losartan for 30 days in adults.
As with all other steps, abnormal labs should be redrawn at the completion of therapy. Blood pressure needs to be closely monitored.
Step 12/ Using low VIP to restore immune balance and regulation
Step 12 is the pinnacle of the pyramid. By this time, most patients will already have become much better with reduction or resolution of at least 75% of their baseline symptoms. Some, not all, will require this last effort.
Particularly, if VIP is used to correct multiple gray matter nuclear atrophy (see the 2017 paper on VIP on the Surviving Mold site), the use of VIP brings the most hopeful changes to those with cognitive effects and mold exposure.
**The criteria for use of VIP (vasoactive intestinal polypeptide, a peptide hormone) includes a normal blood test for lipase; a negative culture for MARCoNS; a normal HERTSMI-2; and a normal VCS test.**
**VIP is not appropriate for patients who still have significant exposures or MARCoNS. It won’t work.**
A HERTSMI-2 (building index score), plus appropriate labs and testing will also be run. These tests will document if the patient’s body has been relatively cleared of toxin, there is no major exposure and, indirectly, that MSH is moving in the right direction. Passing these tests at this time demonstrates the effectiveness of the previous 11 steps and the parameters for the final step.
With resolution of the symptoms after VIP treatment, there will be a final check to verify stability off medications.
Through the whole process, as well as when the Protocol is completed, exposure has to be carefully monitored. If there is a new Water-Damaged Building (WDB) exposure during the Protocol, it’s typical to have to go back to the bottom of the pyramid and start over. Needless to say, taking steps to prevent water damage and subsequent mold exposure is imperative.
RECOMMENDED SHOEMAKER PROTOCOL™ RESOURCES:
1/ We urge you to review the SHOEMAKER PROTOCOL™ PRACTITIONER ESSAYS written by Shoemaker trained and certified physicians. You can print them and use them as a reference.
2/ We offer the Shoemaker Protocol™ Proficiency Partners training program:
THE PROFICIENCY PARTNERS ONLINE TRAINING PROGRAM for both prescribers and non-prescribers.
Upon completion of the program, practitioners are added to the Surviving Mold list serve of practitioners. This group of specialists continues to network and brainstorm every day. We also welcome interaction and articles from the certified partners and practitioners on the Surviving Mold site and in our membership club in a guest-expert capacity.
SECTION 2: Member Q&As – Necessary Tests & Steps (Shortcuts, Variations, Duration)
1/ Necessary testing for worsening illness
QUESTION: I was exposed to a water-damaged building for 5 months. I have been experiencing asthma symptoms and fatigue throughout this time. It seems to be getting worse. I am looking for only the most necessary testing to show me where I am in this illness and what to do now.
ANSWER: There are 4 initial diagnostic steps that you can do from home, and are relatively easy and affordable to do, I would suggest you start here.
One of these steps is to determine that you have a multi-symptom, multi-system illness that is indicative of CIRS. A definitive CIRS diagnosis will show you have several symptoms—more than two.
The method of diagnosis of CIRS is published in peer-reviewed literature that is free to users on this site.
Here are the Quick Start Diagnostic Steps in brief (see also below):
- Show you have been exposed to a Water Damaged Building (WDB)
What patients need to be able to show is that they truly do have exposure to water-damaged building/s, as is shown either by presence of visible mold, musty smells or evidence of speciated microbes. Air sampling will not accomplish either of these three different elements. Dust or Swiffer sampling (ERMI and/or HERTSMI-2 available at EnviroBiomics Labs) is the testing system used with the Protocol as it accurately tests for the biotoxins that affect CIRS patients.
- Patients will also need to verify they have a multi-system, multi-symptom illness as represented in the Protocol’s published peer reviewed literature.
Having asthma symptoms and fatigue are commonly seen in patients with CIRS, but true CIRS patients have far more than just two symptoms. (See a quick-look symptom checker below or an expanded roster in the downloadable Quick Start Guide).
- Take the online Visual Contrast Sensitivity Test for an initial CIRS diagnosis and confirm symptoms.
- Once the initial CIRS diagnosis steps have been accomplished, it’s required to establish care with a practitioner who will follow the Protocol steps and have the laboratory testing done to confirm presence of innate immune abnormalities and provide the initial markers. These lab abnormalities need to be consistent with what has been published in the Protocol’s peer-reviewed literature. Learning if you have the genetic susceptibility (through testing) also informs recovery and relapse prevention.
Shoemaker Protocol™ Practitioners are trained to follow this lab testing process and the Protocol steps, tailored to the patient’s specific case. Or, the Surviving Mold website has a roster of labs to download for your physician.
You may also be interested in #2 below for more information.
2/ Minimum number of tests and steps required
QUESTION: Our adult son has multiple complex health issues possibly related to his HLA DR and a mold exposure. His IgE is quite high and he has extreme eczema. What is the fewest number of tests needed?
ANSWER: If you haven’t already received a confirmed CIRS/mold illness diagnosis, the initial diagnosis is convenient, affordable, and easy to perform, consisting of four basic steps that can be done without a practitioner’s assistance. This process will provide you with enough information to determine whether you need to pursue laboratory tests and additional assessments for a definitive diagnosis. (Refer to the four steps outlined in the library category.)
Once you have confirmed Chronic Inflammatory Response Syndrome (CIRS), it is highly recommended to seek care from a practitioner specializing in the Shoemaker Protocol™. Alternatively, you can guide an attending licensed health care practitioner to the Practitioner Resources and Lab Testing Roster available on the Surviving Mold site, where essential resources are provided.
The diagnostic lab roster of the Protocol is comprised of the basic testing needed to give definitive diagnosis, evaluate the necessary biomarkers, understand the specifics of your case, and begin treatment.
What we look for in the laboratory studies includes:
HLA, MSH, TGF beta-1, C4a, MMP-9, VEGF and a T regulatory cell assay. I will also add ACTH/cortisol and ADH/osmolality if MSH is less than 35pg/ml.
It's also important to recognize that treating CIRS is a comprehensive process that involves more than just laboratory testing and removal from exposure. CIRS is a multi-system, multi-symptom illness linked to genetic susceptibility. Further, "toxicity" is only one aspect of this complex illness, and initial diagnostic testing will identify affected areas, establish a baseline for biomarkers, and reveal genetic factors, among others.
Each aspect of the illness must be tested and treated methodically and sequentially to achieve recovery. Each step strategically targets the next “layer” or aspect of the illness and is addressed accordingly. You cannot determine the need for subsequent treatment steps until you have completed and resolved the previous one. Most individuals with genetic susceptibility will require more than just the first steps, which involve removing the patient from exposure and using Cholestyramine (CSM) or Welchol to eliminate the initial toxic load. (See the Shoemaker Protocol™ steps listed in the library category and the Certified Practitioner Essays for more information.)
The lab roster also provides the health basis to monitor as we progress through the steps of the Protocol, and to determine when resolution of each step, and ultimately the sickness, is obtained.
It is essential to conduct this testing in close collaboration with a Shoemaker Protocol™ Practitioner or a physician who strictly follows the Protocol in the correct sequence. They can also evaluate whether it would be beneficial for you to receive a NeuroQuant assessment to examine the inflammatory effects on the brain, genetic assessment testing, or other relevant tests.
The steps needed will depend how this illness is affecting your son, and to what degree. Only taking each step, one at a time, will reveal the number of tests needed.
Ultimately, the final step—VIP treatment—can yield transformative results for those in need. However, it’s important to keep in mind that this treatment will only be effective when preceded by the prior steps delivering adequate conditions, plus complete removal from exposures.
Skipping steps, especially in a complex case, is never a good idea. In the long run, committing to each step without taking shortcuts will be the most efficient path back to health.
For those with longer duration illness without treatment, such as his possibly could be, the approach to therapy must include consideration of long-term correction of the genomic abnormalities that he is likely to have.
Once a patient reaches recovery, staying vigilant against re-exposure is crucial for maintaining lasting health and should become a way of life. Additionally, utilizing the Protocol medication and measures proactively is beneficial if not essential.
3/ Self-treating with substitutes; symptoms for under a year
QUESTION: I’ve had symptoms including fatigue, stiffness, moderate digestive upset, headaches, and asthma for under a year, do I need the whole Protocol? After moving out from the exposure, I’m starting to detox with activated charcoal. Is there anything over the counter I can take for this? I haven’t found a practitioner to work with the protocol so I’m trying to do this without one. What else can I do?
ANSWER: After you have determined you have a multi-system & symptom illness that fits the symptom profile of CIRS and completed the initial diagnostic steps including the online Visual Contrast Sensitivity Test (VCS), the next step is to establish care with a licensed health care professional who will follow the Shoemaker Protocol™ through the next diagnostic and treatment steps.
The Shoemaker Protocol™ employs lab tests and diagnostic procedures that must be ordered by a licensed health care professional. I do not agree that it is safe or effective for an individual to take on this task without a comprehensive medical understanding of the illness and the Shoemaker Protocol™, plus the ability to order and track labs, tests, and prescriptions. Typically, removal from exposure, adequate rest, and adhering to the treatment steps is more than enough for a patient to handle. Creating a “village” of support is highly beneficial through recovery and beyond.
A trained expert offers invaluable methodology to specifically and strategically treat the multi-symptoms and systems affected in the individual during a time when they are compromised both mentally and physically. Finding specialized Protocol support is the surest and most direct way back to health.
There are numerous Shoemaker Protocol™ trained and certified physicians and practitioners listed on this website, and the list is growing all the time.
The next best recommendation is to point your attending physician to the Physician Resources, including specific lab and test rosters, listed on this site. If your attending physician won’t listen to you, find one who will. General medical facilities are expanding their types of specialists and doctors more and more as well, including R.N.s and D.O.s* who may be more open to the Shoemaker Protocol™. Be sure to inform them of the proven, published, peer-reviewed literature they can find on the Surviving Mold site to support the Protocol.
You mentioned using charcoal, which is not uncommon it seems. However, it has been found that charcoal does not have the binding composition to be effective in treatment of CIRS.
The binding medications CSM (cholestyramine) or second best, Welchol, along with VIP (a neuro-regulatory hormone, used as applicable), as well as the treatments and supplements outlined in this Protocol, have been rigorously tested and reviewed. They continue to achieve optimal results in case after case.
Many other alternatives have been explored, but none have been proven to demonstrate the necessary binding compatibility or regulatory effects. Additionally, the Shoemaker Protocol™ treatments have been found to be safe, effective, and reliable for the vast majority of patients, even for those with the most severe symptoms.
*Doctor of Osteopathic Medicine, a fully licensed physician who practices medicine with a holistic approach, focusing on the whole person rather than just specific symptoms. They are trained to consider how lifestyle and environmental factors affect health and can perform all the same medical functions as a traditional M.D. (Doctor of Medicine).
4/ Treatment Protocol improvement rate & results
QUESTION: What can I expect as far as an improvement rate after use of your protocol at each of the main steps?
ANSWER: The first part of the question to address is that each step of the Protocol is a “main” or “necessary” step until the patient’s symptoms and biomarkers resolve. It can not be known what steps are the main steps for you until you have taken each one, sequentially, until resolution.
(Refer to the Shoemaker Protocol™ overview included above for an average idea of timing at each step.)
What may also provide clarity is that we have looked carefully at people who did not have successful improvement with the 12-step treatment protocol.
The two main sources of problems have arisen from ongoing exposure to the interior environment of water-damaged buildings and incorrect diagnosis due to testing process deviations.
As long as all of the Protocol’s specified labs are drawn, you will have the guidelines to help you follow your illness parameters as you go from one step to another.
If you truly have CIRS, you absolutely must pay proper attention to detail about additional exposures in day-to-day life. While NIOSH says 50% of the buildings in the U.S. are water-damaged, there are times that I think that is an underestimate.
Now that we have VIP and can show improvement in genomics as well as improvement in volumes of structures of the brain by using NeuroQuant, we are in an era where the fundamental mechanisms that underlie this disorder can be identified and effectively treated to the point of symptom resolution.
5/ Case definition for mold illness; labs required for diagnosis
QUESTION: If I have the labs that you suggest run will that show that I have mold growing in my body?
ANSWER: The illness acquired from exposure to water-damaged buildings is not coming from an infectious process of mold of any kind growing inside someone’s body. There have been several patients who I have seen who have had fungi colonizing in sinuses and some patients have had infectious process in the lung.
Those illnesses are separate from the inflammatory response syndrome. The labs I use won’t substitute for a culture. But there is more to this answer. The laboratory data are only part of what is needed to confirm and treat illness.
There must be:
- First, the potential for exposure. If there is water intrusion that is not cleaned up in two days and there is evidence of microbial growth that is shown by presence of visible mold, or the presence of musty smells, plus laboratory confirmation using ERMI or HERTSMI-2 of excessive fungal DNA needs to be identified.
- Second there must be the presence of a multi system, multi symptom illness as reported in peer-reviewed literature, confirmed by a Visual Contrast Sensitivity (VCS) Test
- Third, there must be the specific abnormalities of labs, also as reported in peer-reviewed literature.
- Finally, there needs to be response to therapy.
Each of these elements must be documented, not guessed.
What that means is that without exposure to microbial amplification in a building with water intrusion, there can be no CIRS response. Meeting this first step is harder than one might think. Simply being in a building that had water intrusion but was cleaned up within two days will not count as being exposed to a water-damaged building.
The symptoms that patients have will be from at least 4 organ systems and are ones that are not immediate onset or short duration. They are chronic.
Finally the labs that patients have are represented by a table found in the VIP paper that was published in Health in March 2013 (found on the
www.survivingmold website). This table summarizes the presence of lab abnormalities of 1,829 patients. Take a long look at that registry and see how your labs compare.
6/ Treatment resources with low budget & resources
QUESTION: I have had multiple health symptoms since I was sickened following a hurricane. My home developed very high levels of Aspergillus and Penicillium. I moved out and still remain ill. I have multiple lab abnormalities but as I am on disability this time, I do not have resources needed to assess care.
ANSWER: I do not agree that avoiding treatment because of financial terms at this time is justified as your disability is bad enough; you do not need ongoing progression of CIRS to add more injury. Do whatever you can to receive the medical care you need, find a practitioner who will work with your situation and insurance or aid. It is near impossible for those with CIRS to contribute to a full working life until this illness is resolved.
The first area to look at is to make sure your new environment is CIRS-safe through visible inspection and dust sample testing.
It is also important to note, the treatment protocols that I use are not expensive once you confirm you have been removed from exposure. Most insurance companies will cover costs of cholestyramine or Welchol and most of the labs with proper medical attribution. I would suggest that you discuss your lab abnormalities with one of the certified Shoemaker Protocol™ physicians listed on this site.
The next best option is to find an attending physician who will implement and learn about the Shoemaker Protocol™ and strictly follow it without deviation.
It is your right as a patient to advocate for yourself and choose a physician who will listen to you and support your particular health needs through evidence-based protocols such as the Shoemaker Protocol™. This method is published, peer-reviewed, and proven. It has been held to the highest standards of medical research and data gathering.
Point your physician to the “Physician’s Resources” drop down menu on the Surviving Mold homepage, which includes a complete lab roster.
As CIRS is a complex illness to understand, there is also a comprehensive Shoemaker Protocol™ online training for both prescribers and non-prescribers.
SECTION 3: Alternate Testing, Treatments, Supplements
1/ Supplements, taken for detoxing and symptom support
QUESTION: I cannot find a practitioner who will take my insurance and work with the Shoemaker Protocol™ so I’m working with my naturopath as I’m established with her and it is affordable at this time. I’ve removed myself from exposure and am taking detox supplements including anti-bacterial essential oil tinctures and detoxing supplements (as we understand it’s more than just “mold,” including wdb bacteria and the various biotoxins affecting me). I’m also taking a few supplements to support my system and lower inflammation. It’s been a month and I’m feeling moderate improvement at times but not consistently. I’m wondering about taking supplements while detoxing or during the Protocol, and what you advise.
ANSWER: We do get many questions about natural methods and alternative solutions. The first thing to understand is that Shoemaker Protocol™ treatment steps offer a synergistic blend of prescription medicine, supplementation, diet, and hormone regulation, as needed. It targets the underlying cause and supports the system’s functions to operate optimally, minimizing and eliminating possible side effects during this critical time.
The initial “medication” everyone begins with is a binder, Cholestyramine (CSM). It is FDA-approved and has been safely used for over 50 years for lowering cholesterol levels and as a bile acid sequestrant. It is not absorbed into the bloodstream and has a unique affinity for binding with the biotoxins that affect CIRS patients, preventing their absorption and promoting their excretion from the body. There can be common digestive issues with CSM which are easily treated with home or over the counter remedies. Welchol is a second-best option for those with highly sensitive digestive systems.
Next, a note about alternative binders.
Can your practitioner prescribe? CSM, or Welchol is second best if CSM is too much for your digestive system, are to this date the only proven binders that produce reliable results in case after case. This is because they hold the right charge to actually bind the targeted biotoxins from the system. This is science based. The other binders so many try, simply do not hold the right charge to get the job done. If you prefer the purest form of CSM or Welchol, consider visiting a compounding pharmacy.
For CIRS patients seeking a "natural" or affordable solution, the best advice is to follow the Protocol step by step, one treatment at a time. It’s important not to add any supplements or make deviations from the Protocol, as it offers proven, evidence-based results for restoring health. Each step may take a month or more, but it will guide you toward your next phase of health and recovery, without compromising your system or setting you back. You won’t know how many steps you will need until you complete the previous one. It is worth your time and effort to patiently and strictly adhere to this process.
A word about supplements during the Protocol.
While there are many helpful, quality, scientifically validated supplements, one must be cautious about using any substance with CIRS, especially those that can impact the immune system or detox pathways. Even natural remedies can send a CIRS patient into a tailspin.
Supplements, just like medication, can have a powerful effect in initiating changes in the body. When your body’s foundational operating systems are not functioning normally, a substance used to correct, stimulate or increase a process that is already struggling, can have negative consequences.
CIRS patients sometimes feel abandoned by the medical system and turn to alternatives for relief. These patients may take multiple supplements with multiple actions at one time. This creates confusion because it makes it difficult to determine which substance is making the symptoms better or worse. Some of these supplements can worsen an underlying imbalance that exists or overtax a fragile body chemistry.
There is a time and place for supplements. The best scenario is to work with a Shoemaker Protocol™ trained practitioner who can guide you accordingly. Hopefully your practitioner understands what will and will not best work with your system as you proceed. If you are having mixed results it is best to only introduce one treatment at a time, then after a period of time introduce one more, and so on. This way you can determine the effects of each on your system.
Have you pointed your practitioner to the Shoemaker Protocol™ resources on this site including the lab roster? The CIRS-sieged body can not only handle, but improve with each step of treatment. The Shoemaker Protocol™ Essays written by the Certified Practitioners may also be helpful.
Or, in order to adeptly navigate the complexities of the Protocol, more and more Practitioners are interested in the online Shoemaker Protocol™ Proficiency Partners training program, for both non-prescribers and prescribers. It provides a comprehensive overview, plus networking with the other practitioners and more.
Comprehensive training modules on CSM and VIP as treatment and prevention are also available for purchase.
2/ Urine Testing
QUESTION: I was wondering if there are any resources on SM on interpreting results from urine metabolites testing for mold toxicity.
ANSWER: There is no interpretation for urine analysis as it is not used in the Protocol and Dr. Shoemaker doesn’t support urine testing. There is no conclusive data. There is information on the SM website regarding using that testing in an article called Junk Science. You may also be interested #X below which explores the topic of junk science.
Because CIRS is a complex multi-symptom, multi-system illness, it only makes sense that accurate diagnosis will include more than any one test. The Shoemaker Protocol™ testing process relies on several specific lab test abnormalities as well as a Visual Contrast Screening (VCS), HLA-DR genetic testing, and a specifically ordered NeuroQuant test.
“As far as mycotoxins testing in urine go, I look forward to the day when we will see a monoclonal antibody, not a polyclonal antibody, such that we can actually make clear differentiation of individual breakdown products of toxins and similar epitopes. For example, it is clinically important to see if ochratoxin A, ochratoxin B and ochratoxin ester levels are. I don’t see anyone’s urine test doing that. Without a monoclonal antibody, we can’t really say what the urine test is telling us except that something is triggering an antibody. Does that mean the person is ill? Not ill? Exposed? Not exposed?” - Dr. Shoemaker
3/ Sauna
QUESTION: Will an infrared sauna help with the detox process?
ANSWER: No. Hot saunas usually make people feel great so I have no qualms about suggesting use of saunas provided you avoid dehydration. I am aware there are many claims, primarily from environmental medical physicians, that infrared saunas do magical things. As you might expect, I asked to see confirmatory before and after data. None has ever been produced.
4/ Biotoxin Binders; Pectasol
QUESTION: My primary physician has prescribed Pectasol for my wife who has early onset dementia, felt to be due to biotoxin exposure. Will this work?
ANSWER: No. There is no data published anywhere showing benefit of Pectasol as a replacement for cholestyramine and Welchol, the medication used as a binder in an initial Shoemaker Protocol™ step to begin the detoxification and recovery process. If there are problems with CSM, typically digestive, Welchol tends to be easier on the system. Seeking out the pure compounded version is another option (from a compounding pharmacy). Although Welchol takes longer, it does produce results. These are the only two binders that have been proven to work to date. Also, the low dose VIP protocol can also provide the necessary results in a later step in the Protocol, as needed.
Begin by familiarizing yourself with the Shoemaker Protocol™. Resources are available for your attending physician on the site, or we recommend working with a Shoemaker Protocol™ practitioner or partner.
Information pertaining to this topic can be found in chapter 10 of the textbook, “The Art and Science of CIRS Medicine.”
5/ VIP and CSM replacements
QUESTION: Are Monolaurin and Bentonite clay suitable for natural replacements for VIP and cholestyramine?
ANSWER: The search for natural compounds that would serve as binders for biotoxins has been continuing for over 25 years. To date, there is nothing published that shows benefit in CIRS including those referenced above.
6/ Zeolites/CSM replacement:
QUESTION: Have you investigated or heard any reports on using Zeolites instead of cholestyramine?
It is well established that Zeolite will bind to positive charged metals but will not bind to the negative charged ions making rings in biotoxins. Therefore it is not an effective binder for treating CIRS.
7/ Cholestyramine, substitute with Cholestepure.
QUESTION: Can Cholestepure be used for substitute for cholestyramine?
ANSWER: No. It is not an effective binding agent but a metabolizer.
8/ Cholestyramine, taken in combination with other binders.
QUESTION: Can I mix cholestyramine, activated charcoal and bentonite clay together without them binding to each other?
ANSWER: I have no data on mixing those three elements together and naturally have no data to suggest possible benefit. I rarely think it’s a good idea to do human experimentation with three variables that cannot be controlled.
(Also see question #1 in this section for more information.)
9/ CIRS treatment, blood testing for antibodies
QUESTION: I have been diagnosed with CIRS based on the exposure to the interior environment of water damaged buildings. My HLA is positive; my TGF beta-2 is 7600, MSH is and VEGF low at 22. My C4a was not tested in the correct lab. I have had blood testing showing antibodies to mold (type unspecified). I have low IgG levels. What should you recommend I do?
ANSWER: I would recommend that you treat the inflammatory basis of your illness after you have been removed from exposure and then re-evaluate as time goes by to be sure that your labs have reached levels that are equal to controls.
Some patients do begin the binder process with CSM or Welchol while they are still exposed, but until you remove yourself from the exposures, it won’t be fully effective nor will the rest of the treatment steps.
Blood testing for antibodies for mold is at best a crap shoot and is not associated with any confidence with this illness.
The treatment protocol that this group has used with great success over the years is spelled out in the paper on VIP published in Health in March 2013. This paper is available as a free download from “Resources” on this website.
The discussion of the treatment protocol is featured in the protocol essays written by certified physicians in their section found on this site.
10/ Diagnosis, mycotoxins, negative urine and Lymes testing
QUESTION: I took your online test which revealed I was positive for mycotoxin poisoning. I had urine testing done; the results were negative for mycotoxins. I have been ill for two years in our 5-year old house. Multiple species of fungi were identified in an area of an ongoing leak. I have had fungal antibody testing that was negative. I have had six Lyme tests together with an evaluation with an infectious disease specialist who said that I did not have an infectious disease. Have you ever seen a case of someone who had mycotoxin poisoning but the tests were negative?
ANSWER: If I could do one thing for you, it would be to remove the idea that inflammatory response syndromes are due solely to toxicity or poisoning from mycotoxins.
When diagnosed with CIRS, it includes an HLA-based genetic susceptibility. What we see inside a water-damaged building is a diverse array of compounds that can create inflammation, and for those with the susceptibility, such inflammation is chronic and persistent. The initial genomic effect is that the body does not auto-release these compounds, which are normally released in those without this susceptibility.
In addition to fungi which can produce mycotoxins; and mycotoxins can have genomic effects together with activation of innate immune receptors, there are bacterial toxins; toxins made by actinomycetes; and the real possibility exists that mycobacteria species are also making mycotoxins.
So, the problem is not mycotoxins alone. It is worse in that beyond these fungi, there are other agents at work that are in my opinion of far greater consequence to the body.
As far as the testing you have had done, I see no validity in using antibody testing to diagnose any CIRS illness. As such antibodies, even if they are monoclonal, which is never the case in fungal antibody testing, have nothing to do with innate immune responses and furthermore, do not show when an exposure occurred (assuming the lab is correct, an assumption that is usually not substantiated).
The tests you are basing your information on, the urine and antibody testing, will not tell us if one was made ill by such exposure. I do not know which tests were run to indicate Lymes, so I cannot comment on these.
Since your VCS test is indicating CIRS, I recommend following the Shoemaker Protocol™ diagnostic process, starting with confirming exposure to a water-damaged building and also that you have a long-lasting multi-symptom & system illness. (See the symptom roster and 4 quick start steps included below.)
The next step is establishing care with a Shoemaker Protocol™ Practitioner (see the rosters on this site) or with a practitioner who will follow the Protocol to confirm CIRS-WDB diagnosis and continue the Protocol treatment as applicable. Removing yourself from exposure is the next step that must be taken once your diagnosis is confirmed with a specialist.
THE 4 INITIAL DIY DIAGNOSTIC STEPS:
“Surviving Mold begins with knowing what’s wrong and… having the right plan. This means that mold sickness patients need to both listen and learn, two functions they often no longer perform well. Having the right plan means being patient, because a step-by-step confirmed multi-system mold illness treatment process doesn’t allow anyone to skip steps or be creative and do things differently.
It means ignoring what you heard from a brother-in-law that he heard in a talk on the radio; or read in a blog written by some self-anointed expert based on their own experience, by anecdote or best guess, or read on a web page written by someone trolling for your money. All those pitfalls are out there and discernment is called for more than ever.
Living this plan demands attention to detail, too, but in the end, all this listening, learning and doing, slowly brings back a life filled with meaning and fullness, vitality and insight as these therapies (all tested in IRB-approved clinical trials) correct each system and susceptibility that contributes to the immunologic disease often called mold sickness.”
STEP 1: Test and confirm the suspected water damaged building affecting you.
“The first step is to confirm that there is a microbial problem related to the water intrusion.” Dr. Shoemaker
This is an important initial step because removal from, or remediating the environment to “safe” microbial level is crucial for fullest, lasting recovery, and simply, for the Protocol to work.
You will also pinpoint the organisms affecting you, to what degree. Plus, you’ll have a reference point as to the “unsafe” level, as you work to recover and create a safe environment for you.
Test Kits are available at EnviroBiomics Labs. Dr. Shoemaker helped develop the “Shoemaker HERTSMI-2” to pinpoint the “Big 5” organisms that contribute to CIRS. The test is effective and is available at a lower cost.
This top-notch, specialized laboratory provides results you can trust, educational guides, plus highly specialized, helpful customer support.
See also the free downloadable HERTSMI-2 Scorecard available at survivingmold.com.
STEP 2: The next step is to confirm that you have a multi-system, multi-symptom illness.
This can be accomplished by checking, verifying, and documenting the symptoms you experience. You can check your symptoms below in the resources section. See the Quick-Look Symptom Roster (below) or an expanded list in the downloadable Quick Start Guide or 2013 Paper on VIP (links below).
3: Next take an online Visual Contrast Screening (VCS) to obtain an initial pass/fail CIRS diagnosis within minutes.
You will receive a printable report to review with your physician and/or your Shoemaker Protocol™ Practitioner. It will also provide a base from which to continue tracking your recovery journey.
At this point, if you show you have the VCS deficit, a confirmed building, and multiple symptoms, it’s time to estabilish care and proceed with the definitive diagnosis to confirm the specifics of your case.
If you show you have a VCS deficit and multiple health symptoms then a Shoemaker Protocol™ practitioner or your local physician can assist you by ordering the subsequent labs needed to confirm your diagnosis as a chronic inflammatory response syndrome (CIRS).
“ If your VCS test is normal and you only have a couple symptoms, you probably are not going to be a person who has a CIRS.
If, however, you have a multi-symptom, multi-system illness with a VCS deficit (and the screening on the site will tell you) then I would recommend that you proceed with the protocol diagnosis pathway and have the next labs done. See the lab roster included on the Surviving Mold site for your practitioner to follow.
If you have questions on what to do, this would be an occasion where you would be well off to consult one of the practitioners trained in the Shoemaker Protocol™ listed on this site.” ~ Dr. Ritchie Shoemaker’s reply to a Membership Q&A
4: Make a Definitive Diagnosis and Establish Care with a Shoemaker Protocol™ Practitioner (or, next best, one who will stringently follow the Protocol steps).
After you have a confirmed CIRS diagnosis, it is important to remove the patient from WDB exposure for treatment to be effective.
The definite diagnosis will begin with a detailed and comprehensive history and physical exam. Specific diagnostic tests.
A full battery of labs should be done after your symptom roster is confirmed and compiled and a visual contrast sensitivity test (VCS) is performed.
It’s highly advantageous to find a Shoemaker Protocol™ Practitioner or Proficiency Partner to work with you when dealing with this complex illness.
The next option would be to point your attending physician to the “physician resources” section and the testing and lab rosters available at survivingmold.com. You have every right as a patient to advocate for yourself and find a practitioner who will assist you in using the published, peer-reviewed and well-proven Shoemaker Protocol™.
The highest guidelines of evidence-based research and information are here. You do not have to guess. If these initial steps are confirming the initial CIRS diagnosis, starting here will save you time, money, and quality of life in the long run, rather than trying various doctors and methods looking for.
The Protocol pathway will determine, step by step, the exact treatment you need for your case, eliminating guesswork. You may be a case that only needs the initial treatment steps, or your case may be more complex, and you will need to follow the treatment all the way through. Only taking the Protocol step-by-step, lab-by-lab, will you know what your case and treatment entails.
THE CIRS SYMPTOM CHECKER:
Because CIRS affects multiple systems in the body, patients will exhibit several of these common symptoms:
♦Fatigue ♦Weakness ♦Aches ♦Muscle Cramps ♦Unusual Pain ♦Ice Pick Pain ♦Headache ♦Light Sensitivity ♦Red Eyes ♦Blurred Vision ♦Tearing ♦Sinus Problems ♦Cough ♦Shortness of Breath ♦Abdominal Pain ♦Diarrhea ♦Joint Pain ♦Morning Stiffness ♦Memory Issues ♦Focus/Concentration Issues ♦Word Recollection Issues ♦Decreased Learning of New Knowledge ♦Confusion ♦Disorientation ♦Skin Sensitivity ♦Mood Swings ♦Appetite Swings ♦Sweats (especially night sweats) ♦Temperature Regulation Problems ♦Excessive Thirst ♦Increased Urination ♦Static Shocks ♦Numbness ♦Tingling ♦Vertigo ♦Metallic Taste ♦Tremors
Shoemaker Protocol™ Resource List
Below you’ll find a compilation of some of the most recommended and popular Surviving Mold resources for guiding you, your care team, and your attending practitioner as you recover
(For a more comprehensive list of resources see Membership Q&As, PART 1: About the Shoemaker Protocol™ in this series).
A short introduction and summary of each step of the Shoemaker Protocol™
This short guide explains and takes you through the initial Shoemaker Protocol™ diagnostic steps. Get started right now, and get answers, no doctor appointment required.
Dr. Shoemaker has trained hundreds of practitioners in the Shoemaker Protocol™, and that number continues to grow worldwide. Choose from Certified Protocol Physicians or the Proficiency Partners to find one who can manage your case. Telemedicine options are now widely available.
Our “Physician’s Resources” tab on the Surviving Mold Home Page has the necessary resources for your attending physician to guide you through recovery with the Shoemaker Protocol™ (includes the Shoemaker Protocol™ Lab Roster).
The Surviving Mold Site is full of Shoemaker Protocol-based information and resources, including a Patient Resources section, Group Support offerings, and a Search Bar feature that is very helpful, too.
One of the Shoemaker Protocol’s initial diagnostic steps includes appropriate building testing, either by HERTSMI-2 or ERMI done in your current home and/or other frequently visited buildings, to determine what building is affecting you. This report will also identify which specific types of biotoxins are present, and to what level. You will have information that will inform your recovery and maintenance journey ahead.
Protocol-Related Published Papers & Information
EXPERT TREATING PHYSICIANS CONSENSUS OF 2010 >
One of Dr. Shoemaker’s most-referenced papers provides evidence to support a cause-effect relationship between exposure to the air and dust in water-damaged buildings (WDBs) and a chronic inflammatory response syndrome (CIRS) that is linked to certain genetic HLA haplotypes.
“VIP CORRECTS CIRS…” PUBLISHED PAPER, 2013 >
Review the paper published on use of VIP to learn of its revolutionary effects on the illness, and more. This paper has labs and p-values (statistics) for 1829 mold patients together with nearly 500 controls.
CONSENSUS STATEMENT FOR MICROBIAL REMEDIATION 2020
This document is a consensus statement that expands on existing professional society recommendations by including guidelines for remediation of buildings to be occupied by known, sickened patients.
WHO GUIDELINES FOR INDOOR AIR QUALITY >
Featured Resources

Frequently Asked Questions Volume 9 (2023)
Beginning in 2011, a Physicians Section of Survivingmold provided a forum for discussion of issues regarding mold, Lyme, chronic inflammatory response syndromes and more. Part of the forum included a dialogue on common questions that have importance.

Frequently Asked Questions: Volume 8 EBOOK (2023)
Beginning in 2011, a Physicians Section of Survivingmold provided a forum for discussion of issues regarding mold, Lyme, chronic inflammatory response syndromes and more. Part of the forum included a dialogue on questions that have importance for physicians...