As I See It- Differential Diagnosis

Scott W. McMahon, MD
March 5, 2014
As my children see it, their father is just an old fogie! I have been a doctor for nearly a quarter of a century, almost longer than any of my kids have been alive, so I guess that just makes me old in their eyes. Perception, it appears, makes up a tremendous part of each one of our individual realities. Our individual realities make up much of what we consider truth. And though I turn 52 this week, I perceive myself as being very young – I feel like I’m 20 to 25 years old. Even though I may age chronologically, I will continue to perceive a younger me because there is no way I am going to see myself as an old fogie!
While perception has its place, I also believe in an absolute Truth. I capitalize the “T” in absolute Truth to distinguish it from the personal truth of my life made up of my perceptions and my experiences. My personal truth differs from your personal truth and that is OK. My perceptions and my experiences differ from yours so my personal truth, the truth of my life, will differ from yours. You may not believe in an absolute Truth. That’s OK too. That is part of our individuality. Personally, I find comfort in an absolute Truth, because I believe that without some unassailable standard, ultimately and invariably, the standard by which people judge a matter, or another person, becomes their own personal truth, their own morality or “what would I do in that situation”. I am not qualified to judge your life, nor is my life sufficiently pure to be the standard. I respectfully submit that you are likely not qualified to judge my life either. I am thankful for absolute Truths like we shouldn’t murder, we shouldn’t steal. They are the basis for our laws and the fabric upon which our societies are woven.
Being a practical person, and without getting into metaphysical, philosophical or theological debates, I can give several practical examples of the existence of absolute Truth found in our material world. In the delightful city of Roswell, right now as I am typing, the sun is up. For every person in Roswell that is the absolute Truth. Even a blind person in Roswell, who cannot see the brightness, can feel the sun’s warmth and know it has risen. It doesn’t matter that it may be dark wherever you are, or that the clouds in Roswell are darkening the sky, or even if there is an eclipse, the sun is either up or down. In Roswell, it is currently up. Also, if it is raining over the entire city, it is raining is Roswell, no matter what someone else’s personal perception may be. Further, just because someone hasn’t been to New York City, their personal lack of experience and perception does not invalidate the existence of the Empire State Building. A final example of absolute Truth is this, Chronic Inflammatory Response Syndrome (CIRS) exists as a treatable entity, regardless of whether or not your personal physician believes in CIRS or believes all your symptoms are in your head.
These examples are practical because they help us live our lives. I like practical. Practical is useful for decision making and life is all about making decisions. The metaphysical and philosophical arguments against absolute Truth are based in the impractical, which, to me, makes them irrelevant. Practically speaking, if the sun is up, many of you will wear sunglasses because the bright sunlight hurts your eyes. If it is raining, you will grab an umbrella. Existential discussions are meaningless when you are getting soaked in a downpour. I think you get the idea.
What does this have to do with CIRS? People either have a particular disease or they don’t. It is not subject to personal perception. There is an absolute Truth in that. Just because Aunt Mildred doesn’t believe you are sick does not change the fact that you feel terrible all or much of the time. Metaphysical arguments don’t mean anything to you as a suffering patient. You have a particular disease or you don’t. If you are a physician, you can either help a sufferer or you can’t. Whether patients receive the correct diagnosis or not, however, is subject to the practitioner’s experience and perception!
Put another way, in medicine, we only see what we know. Physicians and various mid-levels can only diagnose that with which they are familiar. If they were not taught about a disease entity, and they don’t take the time to keep learning about new ones, they inevitably will diagnose people incorrectly. It is an inescapable fact and the practice of this principle causes many of my patients to have seen 10, 20 even 30 physicians before they learn what is really causing their illness – CIRS. This sad truth also highlights the need for objective findings in the differential diagnosis (DDx) process of many diseases!
The multi-system, multi-symptom illness known as CIRS can affect nearly any and every system of the body. If your provider focuses on the primary or secondary symptoms – the ones you complain the most about – invariably the wrong diagnosis will be made. For example, if you take 4 patients who all suffer from muscle pains, chronic fatigue, strange neurologic symptoms and recurrent stomach distress, with none of these 4 patients having any objective evidence which most doctors would consider standard, 9 times out of 10 these patients will come away with 4 different diagnoses from most practitioners based on the patients’ differing primary complaints. The patient with very extreme muscle pains will be told she has fibromyalgia. The patient who complains mostly of fatigue will be diagnosed as chronic fatigue syndrome (CFS). The patient possessing primarily strange neurologic symptoms leads to a label of multiple sclerosis (MS). Finally, inflammatory bowel syndrome (IBS) is the disease du jour for the patient whose abdominal symptoms are of primary concern. Each patient has the same 4 symptoms but each is given a different diagnosis… or multiple wrong diagnoses! Most likely, each patient has CIRS and none of the other 4 mentioned maladies. And yes, I can prove that, with a handful of objective lab tests Dr. Shoemaker put together and which most doctors neither order nor understand!
“Five different doctors come up with five different diagnoses based
on the same evidence.”
Gregory House, M.D.
“House, M.D.”, Episode 1
I have recently started watching “House, M.D.” reruns on Netflix with my wife. I typically avoid television doctor shows because their failed flirtation with reality makes me mad. But my wife is wonderful, and she really wanted to watch it, so I caved. Dr. House is possibly the most well-known doctor in America (without a website). He is my son’s generation’s Marcus Welby, M.D. Dr. House is a brilliant diagnostician but suffers from a terrible bedside manner. Though I would never treat human beings like he does, I do admire Dr. House’s approach to diagnosis. He always sticks to the time honored DDx process and, because of this practice, he and his team eventually get the right diagnosis and usually save the patient. Dr. House is very practical but he also thinks outside the box. He had one of his team sniffing an enigmatic patient’s home carpet for mold in the first episode. Dr. House also says some pretty profound things about the medical profession. In episode 6, he makes the following comment to his team of less experienced doctors.
“I have a headache. It’s my only symptom. I go to see three doctors.
The neurologist tells me it’s an aneurysm. The immunologist tells me
I got hay fever. The intensivist can’t be bothered, sends me to a
shrink who tells me that I’m punishing myself ‘cause I want to sleep
with my mommy… Pick your specialist, you pick your disease.”
This sums up the approach of specialized medicine. This results from a failure to use the DDX process in medicine. This is another reason why my patients see so many providers before they get the right answer.
Admittedly, I too specialize in the diagnosis and treatment of CIRS. I avoid the twin pitfalls of misdiagnosis and missed diagnosis because I actually employ the DDX process and I insist on objective testing to confirm, or disprove, the diagnosis.
Another consideration to keep in mind is that which separates well trained physicians from lay people has changed in the last 20 years. It used to be that doctors had all the access to medical information and patients had very little. The internet has changed everything. Many books, such as Surviving Mold, written for lay people and covering numerous health conditions are also available. Physicians used to know it all. But now there is so much information out there that no diagnostician can keep up with everything. Nowadays patients often know more about a particular topic than their treating practitioner. Internet content and medical tomes are not created equally, however. Each writer has an agenda (even I do) and each author has a differing level of experience and knowledge. You must not believe everything you read!
What still differs between medical professionals and lay people is a factor called “medical judgment”. A physician’s medical judgment is honed by intensive training in critical thinking, years of experience and the time honored differential diagnosis process. Critical thinking allows physicians to read a single patient case report without emotion and to understand that the weight of the evidence presented is not equivalent to a prospective, randomized, double blinded trial with a large number of subjects. The experience of having seen many patients with a given condition, over a lifetime, gives physicians the ability to assess severity, recognize variants, predict outcomes and order therapy with some degree of proficiency. Both of these measures affect perception. The DDx process is the method by which doctors ascertain the absolute Truth regarding patients and their true disease state. What is the proper diagnosis? How do we prove it?
The DDx process, to my knowledge, is taught to every student in every American medical school and is laid out in every general medicine text. It is the fundamental thought process used to determine the cause of illness so that the appropriate workup and therapy can be instituted. Proper performance of the DDx requires the practitioner to obtain a thorough history from which a mental list of all possible diseases is generated. (If you don’t know a disease, you will not think of it!) I was taught that careful history alone will reveal the proper diagnosis in 75% of all patient visits (even without a physical exam or lab testing). Physical examination is designed to rule some diagnoses out and strengthen the likelihood of others. Lab testing, when necessary, is intended to further refine the list and prove the diagnosis in some cases. The purpose of this process is to evaluate every possible disease which could cause the patient’s complaints. A number of maladies are considered possible until one is exclusively ruled in and all the others ruled out. Extra consideration is applied to unlikely but exceedingly severe diagnoses, such as cancer, so as not to miss a major malady. With experience, practitioners are able to develop mental patterns of illness allowing them to evaluate a wide array of potential illnesses and syndromes in moments. But experience, without keeping current, causes practitioners to miss newly described entities. We only see what we know. If we don’t know CIRS, we as physicians will miss it. A missed diagnosis does a patient no benefit. I missed CIRS any number of times over many years until my eyes were opened. Now I know CIRS in adults and I see it everywhere, because it is everywhere! Because I now see it, I can now treat it.
I remember in my pediatric training, at a Top 10 pediatric residency program, being taught that most children with recurrent abdominal pain had something called “functional pain”. Some kids had constipation, some had gas and some had urinary tract symptoms. A rare few had cancer and others, the ever exciting, but rarely provable, “malrotation”. Almost everybody else, which really means “most kids with abdominal pains”, had functional pain which meant the pain was real but was not due to an organic problem (actual illness with identifiable pathology). Instead, these children were all perceived to have pain to meet a psychological primary or secondary gain. A primary gain meant that they wanted to get out of a test at school that day so they had abdominal pain “as a coincidence”. Secondary gain meant that subconsciously they wanted something, like more attention, so their body unconsciously manifested this pain to get their need met. For years I diagnosed kids like this and taught this psychobabble to their parents. Uggggh! This is what medicine without objective testing looks like. Unfortunately, many illnesses, such as Lyme disease, with and without “co-infections”, are diagnosed and treated in this same way today.
After I was out of training a few years, pediatricians started talking about lactose intolerance and H. pylori causing peptic ulcer disease in children as new reasons for recurrent abdominal pain in kids. A few more children were able to get therapy, but still most had functional pain (a.k.a., it’s all in your head). I’d send them to the pediatric gastroenterologist who would have little additional to say. Enter Dr. Shoemaker and CIRS. I still perform all the routine tests on my pediatric patients with chronic abdominal pains. But when those tests all come back normal, and you know, they usually do, I screen these kids for CIRS. If the screen is positive, and it usually is, I work them up for CIRS. Voilὰ, they almost always have 4 or more abnormal biomarkers. I treat them with Dr. Shoemaker’s protocol. Their chronic abdominal pain goes away. My office’s success rate in chronic abdominal pain remission hovers near 95% (unpublished data)! I haven’t seen a case of “functional pain” in years. We see what we know. We treat what we see. I know CIRS in children and I see it all the time. What I used to call functional abdominal pain, which was relatively untreatable, is now almost always CIRS which is easily treated!
Medicine evolves and grows. I have been in medicinelong enough to remember when fibromyalgia, CFS and IBS were fledgling thoughts as illnesses. They are still considered “wastebasket diagnoses”. Basically, this means all other diagnoses have been ruled out by the DDx process, but these diagnoses cannot be ruled in or out definitively because they do not have any objective findings that prove they are the causative problem. It is for this reason that these diseases were, and still are, controversial in some circles. The lack of objective findings, such as blood or imaging tests, which confirm these illnesses, has even today caused many physicians to not believe such diagnoses even exist. They are impossible to “rule in” because there is no known confirmatory objective data. Conflicting thought in medical journals leads some to believe that these illnesses are somatoform, i.e., “it’s all in your head”. That perception leads to referrals to the psychiatrist for these organically ill patients! It is “functional abdominal pain” for adults!
Back in their infancy as diagnoses, these three were fairly easy to distinguish from each other. Fibromyalgia caused profound muscle pain and usually was coupled with significant sleep disturbances. CFS patients had profound fatigue. IBS patients had recurrent abdominal distress, with or without diarrhea, resistant to standard diagnostic procedures. Another diagnosis, multiple sclerosis, predates my medical career by more than 130 years. It too has historically been poorly characterized. Patients with MS typically had recurrent multiple strange neurologic manifestations, such as unusual pain patterns, numbness and tingling, muscle weakness etc. Each of these 4 diagnoses suffers from relatively little or no objective testing which confirms the diagnosis definitively. Where such testing exists, as in MS, relatively few patients diagnosed with the disease actually possess the positive finding. These 4 diseases had distinctly different patterns and were clearly 4 different entities (if you accepted them as diseases). Pictorially they could be represented as in Diagram 1:
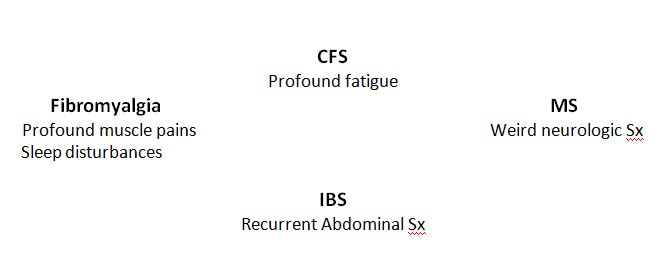
Diagram 1
It seemed pretty straightforward 20 years ago. But a review of the current literature (or any patient friendly websites regarding any of these diseases[1],[2],[3],[4],[5],[6],[7],[8]) reveals a clear blurring of the lines. CFS, Fibromyalgia, IBS and MS have all now been imbued with other associated symptoms making the diseases all look very similar. Please see Diagram 2:
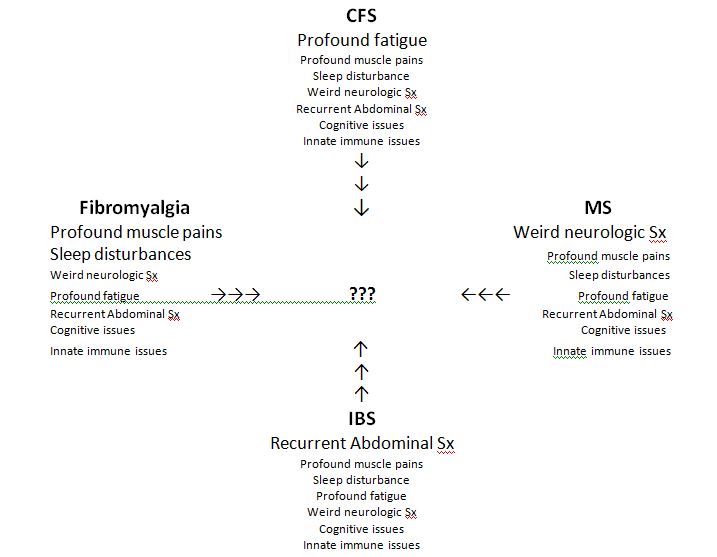
Diagram 2
Indeed, the only thing differentiating these illnesses from each other nowadays is their primary Sx. As elocuted in the introduction, the approach of focusing on one major symptom will cause the general practitioner and the specialist alike to miss the forest for the trees. The patient will be misdiagnosed with fibromyalgia, CFS, IBS or MS, or even combinations of these, but the practitioner will miss the most likely correct diagnosis: CIRS. A missed diagnosis means the proper treatment will be missed too. You, the patient, receive a diagnosis which has no hope and terrible treatment outcomes. That is yet another reason why people will see 30 doctors before they see me!
A closer look at Diagram 2 reveals arrows pointing to the center where several question marks are placed. This indicates that these illnesses (3 out of 4 considered wastebasket diagnoses because of their paucity of objective lab findings) are morphing into one disease. What is that disease? CIRS! Please review Diagram 3.
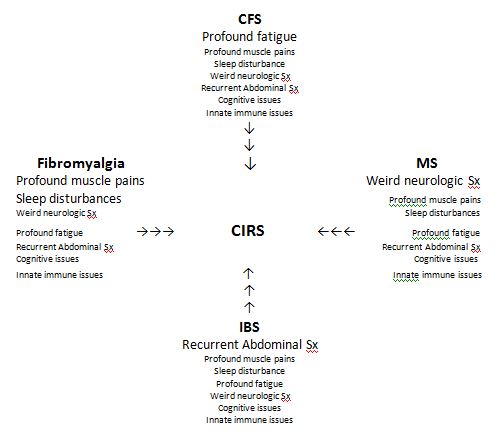
Diagram 3
The take home message is that many patients who have been diagnosed with fibromyalgia, CFS, MS and IBS, or combinations thereof, have been misdiagnosed. They have been treated for diseases which they do not have and they have not gotten better. They typically have CIRS! Don’t believe me? Then do the labs… they will be abnormal for CIRS, but there is little to check for the other illnesses! That’s why they are called wastebasket diagnoses!
I am further astounded athow many adult patients I have seen misdiagnosed by board certified internists! I have seen more patients than I care to count diagnosed with rheumatoid arthritis (RA) who have no objective findings of RA. Yes they have joint pain but a review of their records reveals they have no nodules, no redness, no swelling, no heat at the affected joints, normal C-reactive protein and “sed rate” lab tests, negative ANA and rheumatoid factors and normal X-rays. When I test these patients, they have high TGF-B1’s, low VIP’s, low MSH’s, abnormal genetic haplotypes, high C4a’s etc. When treated with cholestyramine (CSM), their joint pains often resolve completely! These patients were diagnosed with RA, but never had RA, and have been through God only knows how many nasty treatments regimens (NSAID’s, gold, methotrexate, Humira etc.) to control their adaptive immune system when they had an innate immune system dysfunction all the time. I seriously see these type misdiagnoses every single week. Misdiagnosis stems from an incorrect perception of the diagnosing practitioner and a failure to use the DDx process. No wonder my patients have so little hope when I meet them. No wonder they are so thankful when we finish our first session and I have explained to them what is actually going on in their bodies and how they are going to get better.
I have seen patients who have been misdiagnosed with lupus, Lyme disease, “chronic Lyme disease”, hemochromatosis, IBS, fibromyalgia, MS, CFS, RA, chronic pain syndromes, peripheral neuropathy, panic attacks, migraines, migraine equivalent syndromes and a lengthy list of other diseases by well-meaning and presumably well-educated and trained physicians. I say misdiagnosed because evaluation of these patients’ extensive medical records showed no objective evidence for the misdiagnosed malady but the appropriate workup for CIRS revealed numerous abnormal objective tests. Why were these patients misdirected? Their practitioners failed to properly use the DDx process; they focused on one symptom instead of the entire constellation of symptoms and they only saw what they knew. They didn’t know CIRS, so they didn’t see it. But, by God’s grace, I do know CIRS, and the treatment protocol Dr. Shoemaker developed is very effective when followed properly.
I have also observed that patients bring their perceptions into the process. It can be very difficult to convince an ill person, or their family, that the previously applied label of lupus, or fibromyalgia, or MS, or Lyme disease etc. is not accurate based on lack of objective evidence, and that they had CIRS all along. Even when the CIRS labs come back abnormal, it can be hard for them to accept. Even when treatment protocols by the previous practitioners have failed, and patients show marked improvement with Dr. Shoemaker’s protocol, some patients cling to the previous (mis)diagnoses. I do get it. These poor souls have been suffering a long, long time. They have developed relationships over years with other providers who have offered them hope and treatments which, unfortunately, usually didn’t work. I come along and tell them they really have CIRS, I explain how it has affected their body and how Dr. Shoemaker’s protocol will make them better. Of course they have doubt… because everybody before has made the same promises. But our outcomes are amazing and our patients get much better. That is my perception but also my scientific observation. That is why I do what I do. Dr. Shoemaker’s protocol works!
I’ve talked about the perceptions of medical personnel and also patients. Doctors either know this disease or they don’t. If they don’t, patients will be misdiagnosed or missed diagnosed (told they are crazy, or a slacker, or a drug seeker, or that this is a somatoform illness, or that they are a malingerer, or that this is all in their head). Patients have their own perceptions and are often convinced of one or another diagnosis, whether correct or not. The last thing I should mention is the varied perceptions of family, friends and employers.
Family and friends are supposed to care for us without condition, love us through all our trials and generally speaking, “have our 6”. Unfortunately, the people that love us the most often hurt us the most. They don’t understand. They can’t experience what the patient is experiencing. They often judge using the “what would I do in that situation” paradigm. They doubt and disbelieve. They typically believe what the misperceiving doctor says and they think that, “Mary Jo actually looks pretty good, so how could she really be that sick?” Many marriages and other relationships end because of CIRS and the accompanying wrong perceptions. Hopefully this article might enlighten some significant others.
On the other hand, employers tend to fall into three categories. One group wants to do the right thing and will do so regardless of the cost. These are the exception. The next group starts out doing the right thing, then finds out that simple fixes won’t do it. When they realize that minimal remediation of the workspace does not help alleviate their employee’s illness, bosses can become defensive. Relationships get strained and things can get touchy. The third type refuses to believe mold can cause illness and will not do anything to help. They often get aggressive, or passive aggressive, with the ill staff member and look for a way to get rid of “the troublemaker”. Perceptions of the value of right and wrong play a major part in these transactions also. Contradictory information on the internet, and from so-called “experts in the field”, makes gathering the correct information upon which to conclude which is the proper path a more difficult proposition
A misdiagnosis is just as bad as a missed diagnosis! In the end, we as health care providers, patients, family, friends and employers, only see what we know and practitioners only treat what we see. The differential diagnosis process is intended as a standardized method to learn the absolute Truth about a patient’s diagnosis and serves as a protection against misperceptions. Many physicians unfortunately focus on one system or one primary symptom and ignore the DDX process . Most physicians do not know about CIRS, hence they don’t see it or treat it. Fortunately, Dr. Shoemaker is training and certifying a group of physicians that know CIRS and can treat it effectively. Let the misdiagnoses and the missed diagnoses stop, now, and let the healing begin!
[1] http://www.mslifelines.com/pages/what-is-ms/ms_symptoms
[2] http://www.anapsid.org/cnd/diagnosis/goldstein.html
[3] http://www.back-pain-treatment-and-relief.com/fibromyalgia-symptom-checklist.html
[4] http://www.webmd.com/ibs/guide/irritable-bowel-syndrome-ibs-what-increases-your-risk
[5] http://en.wikipedia.org/wiki/Irritable_bowel_syndrome
[6] http://www.neurosymptoms.org/
[7] http://autoimmunedisordershelp.com/innate-immunity-autoimmune-disease/
Featured Resources for Community
Shoemaker Protocol™ Quick Start:
The 3 initial steps to determine if mold is affecting you One of the most common questions we hear is, “how do I know if I have mold illness?” Rest assured, if you’re asking this question, you’ve come to the right place.

AirOasis The #1 CIRS Spring Cleaning Hack
Specialized air purifiers are revolutionizing deep cleaning, no matter the season. They’re a game changer for remediation purposes, too.

CIRS Spring Cleaning Checklist
Living with CIRS means cleaning and maintenance efforts must be ongoing and up to CIRS-safe standards. Spring is a perfect time to do a thorough examination and cleaning of the entire home and create a schedule for the year ahead.
CIRSX Annual Conference June 5-8, 2025 in Tempe, Arizona!
Early Bird Discount ends March 7!
NEW EPISODE! Dr. Shoemaker on Episode #211 of the BetterHealthGuy Podcast!
New Episode! Dr. Shoemaker joins Scott on the BetterHealthGuy.com podcast to talk about the use of GENIE testing in Chronic Inflammatory Response Syndrome.