New Surviving Mold Website Features
We welcome you to take a look at the many new features of our website. (1) We now have hand held VCS kits available for public use (APTitude testing) for those who wish to do multiple VCS tests. Once the simple protocols for hand held VCS testing are in place, and followed routinely, the kit can be used hundreds of times. (2) Videos of Dr. Shoemaker’s recent teaching sessions are now available as well. (3) The Physicians Section provides an opportunity for advanced interaction between Dr. Shoemaker and licensed practitioners to go over issues in diagnosis, treatment and case management of Biotoxin Illnesses.
Dr. Shoemaker will be presenting two days of lectures/talks on October 22-23/2011 in Santa Rosa, California in an event sponsored by Gordon Medical Group. The first day is for patients and the second day is for physicians. The teaching slides and syllabus will be on this site in November. For more information, see the link to the conference.
Three new academic papers are now available for viewing on the site (click here to view). These presentations were made at the 6th International Conference on Bioaerosols, Fungi, Bacteria, Mycotoxins and Human Health, held 9/7-9/9/2011 in Saratoga Springs, NY.
This conference is a continuation of the “Johanning” conferences that have been held since 1994. Organized by Dr. Eckardt Johanning, this venue brings together leading experts in the fields of mycology, building engineering, industrial hygiene and physicians experienced in the field. The conference speakers are truly an international “Who’s Who” in the field of water-damaged buildings (click here for more information).
VIP
Dr. Shoemaker made four presentations at this conference, with the first being the presentation on 18 month follow-up of 20 patients treated in an IRB-approved clinical trial of vasoactive intestinal polypeptide (VIP). These patients were among the most affected in Dr. Shoemaker’s practice. The phenomenal clinical and laboratory improvement seen without significant adverse side effects holds great hope for additional studies on the treatment of the chronic inflammatory response syndrome that is caused by exposure to the interior environment of water-damaged buildings (CIRS-WDB). NOTE: VIP should not be used by physicians unfamiliar with the entire sequence of treatment of the Biotoxin Pathway, however, as benefit of use is not seen for those with (1) ongoing positive VCS scores; (2) presence of multiply antibiotic resistant coagulase negative staph in deep aerobic nasal cultures (insert link to DLM) performed by Diagnostic Laboratory Medicine or any lab using a technique similar to API-STAPH. The negative culture result must be in the medical record before using VIP. Finally, (3) the ERMI score must be less than 2 or HERTSMI-2 score less than 10 (insert link to HERTSMI-2). We are seeing a number of mycology labs performing ERMI with results that basically are impossible, with non-detects (ND) showing up repeatedly that are refuted by ERMI done by Mycometrics. Until we see confirmation of accuracy of the other labs, we can only recommend use of Mycometrics at this time (insert link). Note: there is no financial link between survivingmold.com or Dr. Shoemaker; or any conflict of interest problem regarding this recommendation to use Mycometrics. I am quite concerned at the absence of reliable results found when cut rate ERMI testing is done. But what surprise is that?
T REGS
A second presentation was on T-regulatory cell (T regs) changes in patients with illness acquired from WDB. These cells are integral to the tissue-based (cellular) innate immunity seen in the CIRS-WDB. Low levels of T-regs are seen in untreated cases, especially children, and in those with reacquisition of illness with re-exposure after successful treatment were completed. Higher levels are seen after therapy, particularly with VIP. Interestingly, several types of “disease-modifying drugs,” including methotrexate, used in rheumatoid arthritis and psoriasis; as well as the interferon drugs (Avonex, Betaseron, Copaxone and Rebif) used to treat multiple sclerosis, also drive up levels of T regs. One might reasonably ask if we shouldn’t revisit the mechanism of illness modulation produced by these widely used agents. The test code from Quest for the CD4+CD25+ T reg cells is 56880 (LabCorp doesn’t run it yet). Patients wishing to have this test done (and that is a very good idea) are well-advised to check with their lab before having the test done as we find no other test order is botched by distant labs more than this one. The lab codes on the website are updated frequently but despite current information, often labs away from my catchment area will guess at what the CD4+CD25+ means. And they usually don’t guess right. So take a few minutes before the draw to be sure that there is no gnashing of teeth over failed attempts at blood draws several weeks later.
PHYSICIAN PANEL DISCUSSION
The third presentation was a panel of five physicians discussing various aspects on illness acquired following exposure to WDB. Unfortunately, none of the other panelists had a data base from their personal experience on successful therapies, so the 90-minute session ended up being a discussion of parameters that our group has published. The good news was that one of the panelists, Dr. Eugene Kern, now at SUNY-Buffalo (with Drs. Ponikau and Sherris), and previously chair of ENT at Mayo Clinic (Rochester, Minnesota), wants to collaborate on research regarding the inflammatory basis of the fungal cause of chronic rhinosinusitis and systemic inflammatory responses. This research shows great promise.
HERTSMI-2
The last presentation was made for a panel discussion on ERMI that including Dr. Chin Yang, Dr. De-Wei Li and Dr. Philip Morey. Dr. Yang asked me to produce comments on ERMI from my practice. This investigation of 738 ERMI results led to the Health Effects Roster of Type Specific (fungi producing) Mycotoxins and Inflammagens (HERTSMI, see link on the site). An initial version looking at nine species of Group I organisms in ERMI was refined to five organisms. The acronym for this scoring system is HERTSMI-2. The name curiously sounds like a blues ballad from the 1930’s that was often performed by the Grateful Dead in the 1970’s and 1980’s. This system provides a weighted score for identification of organisms from 60-80% water saturation (Wallemia); 80-90% saturation (Aspergillus penicilloides and A. versicolor); and finally 90-100% saturation (Stachybotrys and Chaetomium). Scores over 15 are 100% associated with reacquisition of illness by previously sickened patients and scores less than 10 are 100% associated with lack of reacquisition of illness. Scores of 11-15 are a “grey area” and more remediation is suggested before entering these buildings. Understanding that nothing in biology is 100%, the ultimate parameter that confirms safety of a given building is re-entry without medication and absence of recrudescence of illness. HERTSMI-2 looks good so far, however.
An example of benefit of use of HERTSMI-2 came from South Dakota recently. A business man was quite ill with a CIRS-WDB, yet his ERMI in his home and office weren’t too bad. He was struggling to improve until his elevated HERTSMI-2 score showed that his office building had all three water saturation ecological zones represented. The building is new construction, without any evidence of roof leak or wicking of water through the concrete slab foundation. On a hill, the building didn’t have a ground water problem either. Investigation of the building showed absence of some weep holes in the brick façade and significant fungal growth underneath. The bottom line in this case is that ERMI is useful but modifications are available that fine tune the fungal DNA results to make the DNA testing into a tight fitting indicator of human health risk. ERMI is a good screen but HERTSMI-2 is the best roster for treating physicians.
GENOMICS
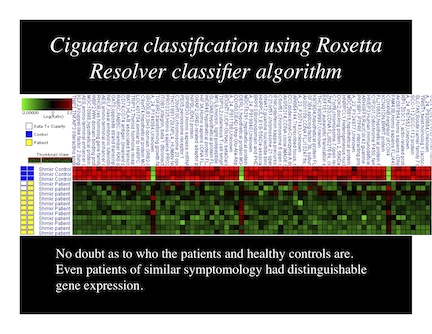
Another new feature of the site is the PAXgene testing program. Talk about the dawn of a new era! We can now send special blood collection tubes to participating physicians to use to collect samples for mRNA analysis. We can actually tell that physician what genes from a targeted group of genes are active and which are suppressed. That information unveils the information needed to guide additional therapy. We have been working on this genomic approach for five years, with spectacular results coming forward everyday. We have funding for a limited number of patients to have genomics testing done within the structure of this program. If your physician is interested, have him/her contact us. An example of this genomic approach seen in cases of ciguatera versus controls is shown here.
LITIGATION/NIOSH HHE
We continue to see the same idiocy from defense interests as before. The same non-science from ACOEM that was sold to the American judicial system as good science in 2002 has been re-released in 2011. Amazingly, the gall of the perpetrators here is that they include no new references at all; include no list of authors; and make no disclosures of conflict of interest. ACOEM 2011 is reviewed in detail on this site (see Ploys and Lies of ACOEM, link). Defense has nothing to refute good science yet they will say anything, and lie they do, to try to avoid owning up to their responsibility.
I’m told the Lanier Middle School case in Fairfax City, Virginia settled recently for close to $2 million. David Wise of Wise and Donahue has won another huge case. This case is one that disturbingly included a biased and wholly flawed report of NIOSH investigators led by Dr. Elena Page purporting to show the school was safe. Drs. Yang and Morey destroyed the basis of Dr. Page’s naysayer opinion about environmental contamination in her defense-friendly publication (note: this is not new ground for Dr. Page). The physician apologist, who was paid over $120,000 by the defense (deposition testimony) to provide cover for the confabulated defense ideas, was unable to provide effective deposition testimony to undermine the massive amount of human health data, including multiple prospective, re-exposure trials accumulated by our group. Still, the school was able to avoid testing the rest of the faculty and staff and no public outcry emerged to demand testing of students.
Yet, one must why NIOSH itself, a Federal agency with a sworn duty to protect workers, would permit such inaccurate and deceptive writing by Dr. Page and her colleagues? Let us not forget, they have done it before (the Scotia Prince Cruises case will be featured in the actual NIOSH irregularities report), so maybe that is standard procedure for the HHE team. I’m sure the conspiracy theorists will note that the ex-deputy director of NIOSH, Dr. Page’s former boss, is a co-author of ACOEM 2002 and is involved with Veritox, a defense-oriented litigation group. Maybe there isn’t any conflict of interest here. But if there is there evidence of conflict of interest, would that impact on what weight courts apply to flawed reporting from government agencies? Are we so naive to think such shenanigans can’t take place? I don’t know.
We don’t know the basis for Dr. Page’s aberrant ideas but to have such work released under the aegis of NIOSH is shocking. Perhaps we will see some sort of government based investigation of such ploys, but I doubt it. In any event, look for the word-for-word review of the HHE on Lanier Middle School together with discussion of the two different reports written by Dr. Page on the Scotia Prince Cruises case, with the Fortier School report discussed as well.
It is too bad that Senator Kennedy isn’t around to ask the GAO to investigate such suspicious activity from NIOSH. We need a lot of Sunshine brought to bear here. Just imagine the impact that exposure of a link of cover-up about mold from NIOSH to CDC and higher-ups in the government (and insurance companies??) would have were it brought to light. For the record, I am not a conspiracy theory advocate.
Having said that, the work from NIOSH in Morgantown, West Virginia continues to be objective and sound in its science. Should anyone else have concerns about malfeasance in duty from the NIOSH HHE team, please contact us at this site.
FOR THE FUTURE
We are working on new diagnostic testing for compounds found inside WDB. We hope to have a device available that will alert affected patients about the dangers of indoor environments. Ideally these devices would be hand-held and would either make a sound or show a color change with exposure to toxigens and/or inflammagens indoors.
We will continue to speak out in favor of truth in science and integrity in medicine and government. We have an ongoing national disaster with the number of moldy buildings in the US, independent of floods and foreclosures. We can provide effective diagnosis and therapy; all of us just have to become involved in protection of human health.